

Tips for Identifying and Improving Sexual Dysfunction in Parkinson's Disease

Wissam Deeb completed his MD in Lebanon at the University of Balamand. He completed his residency in neurology at the University of Massachusetts in 2015. He then moved to the University of Florida to pursue a movement disorders fellowship, and stayed on for faculty until June 2020, when he moved back to UMass where he is an assistant professor of neurology. Dr. Deeb has a clinical and research interest in DBS, Parkinson disease, and Tourette syndrome, and he focuses his career on incorporating technological advancements such as wearable devices into clinical— and everyday care. He also recently published an article in the New England Journal of Medicine on Memory Flashbacks and was the co-author of the new book Living with Parkinson’s Disease. We bent his ear about a topic not discussed enough in Parkinson’s— sexual dysfunction!
I have sexual dysfunction and it is
uncommon in Parkinson’s disease so I
don’t talk about it.


Urinary and sexual dysfunction symptoms are widespread in Parkinson’s disease (PD), though they are rarely discussed—and seldom well managed. In one study (PRIAMO), almost 20% of the individuals with PD reported sexual dysfunction. The most common sexual dysfunction in PD was a decrease in sexual function (such as erectile dysfunction or vaginal tightness), sexual interest (decrease in the libido), and sexual performance (due to stiffness/slowness and possibly mood problems). Less commonly (~3.5%), increased libido and compulsive sexual behavior can occur as a manifestation of impulse control disorder (dopamine agonists)— or from sexual behaviors which can occasionally result from levodopa use. The most common thing we see in our practices is the result of prescribed medical treatments— when using dopamine agonists (pramipexole, ropinirole, and rotigotine).
Besides PD, there are other reasons for sexual dysfunction that can occur with age or other conditions, such as smoking, diabetes, or heart disease. Many medications that can be used for different or related health problems can also cause sexual dysfunction. For example, medicines used to treat depression (called SSRIs), heart failure (thiazide diuretics), blood pressure, and heart rate (beta-blockers) can negatively affect sexual function.
It is essential to bring these symptoms up with your doctor.
2. I have Parkinson’s disease and so sexual
activity should not matter.

Sexual desire and sexual activity remain an essential part of life for both older men and women. Sexual dysfunction for the general population and for persons with PD can be frustrating and very disabling. Sexual dysfunction contributes to a lower quality of life. Indeed, an active sexual life can be considered a surrogate for general health. In the PRIAMO study, men with PD who had “better” sexual activity had fewer problems with their motor symptoms, less issues from depression, and an overall better quality of life.
3. There is nothing much that can be done so why
bother telling anyone.
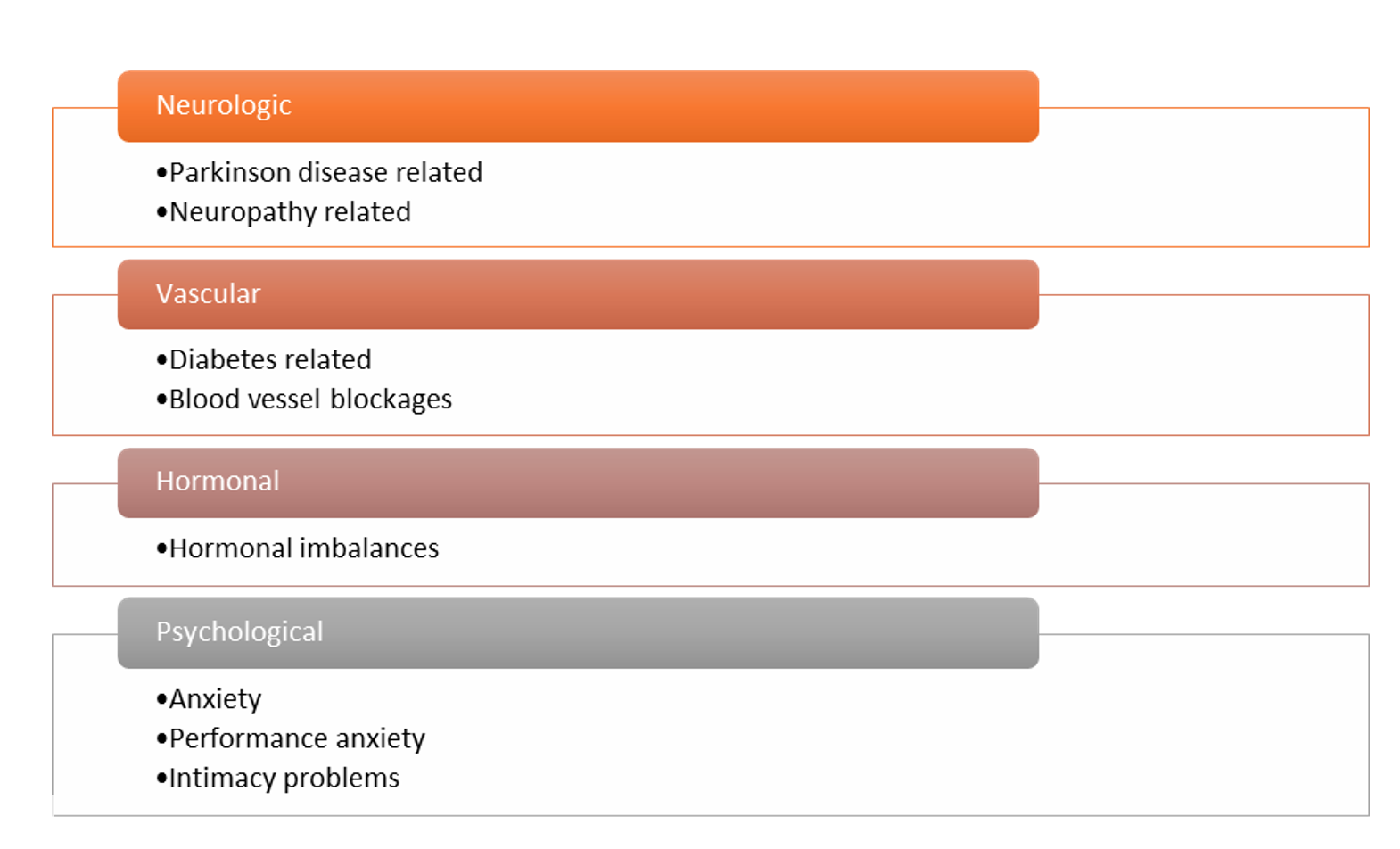
There are multiple reasons for sexual dysfunction. Identifying the cause and constructing a plan with your doctor and healthcare team is the first and most critical step.

Here is a list of what can be done to help
(based on the issue):
Erectile dysfunction and problems with ejaculation
- Are your PD motor symptoms (stiffness, slowness, tremors) well controlled? Poorly controlled motor symptoms negatively affect sexual function, both physically and psychologically.
- Do you take any medications that can negatively impact your sexual function? Review the list of medications with your doctor and determine if some may be causing the problem(s) and if they can be replaced or stopped.
- Discuss medication treatments by mouth. Medications called phosphodiesterase inhibitors (such as Viagra) can improve erection in most people with PD. It is crucial to discuss if you qualify to use these medications. They should not be used if you have low blood pressure or low blood pressure when standing up – a common problem in PD.
- Discuss “injectible” medication treatments. A medication to treat erectile dysfunction can be injected directly into the shaft of the penis (usually well-tolerated and not as scary or painful as you might imagine). The effect lasts from 2 to 4 hours and is safe in people with low blood pressure. It requires hand dexterity to inject, which can be a problem for some people, though the bed partner can inject it.
- Discuss mechanical devices. These include vacuum devices and constriction bands. Please take into account that these devices require varying levels of hand dexterity for use.
- Discuss penile prosthesis. In some cases, following a urological specialist consultation, you might consider a penile prosthesis implantation (as an option). This approach can provide controlled erections without the use of repetitive injections. Surgical intervention is required.
Problems with vaginal lubrication, losing urine during sex, and inability to achieve orgasm
- Have you used artificial lubricants? If you are dealing with decreased vaginal lubrication, which can be associated with reduced pleasure and pain during intercourse, consider using artificial vaginal lubricants.
- Discuss urinary incontinence during sex. First, attempt to void your bladder before intercourse. If this is not successful, check with your doctor— sometimeshyperactive bladder medications can help (and sometimes they can cause confusion and difficulty thinking).
- Discuss the use of medications by mouth (e.g. pills). The use of medications such as Viagra/Cialis can improve sexual function in women and not just in men. Discuss with your doctor if the use of Viagra/Cialis is appropriate. If you deal with low blood pressure, then you should possibly not use this class of medications.
Low libido/low sexual desire
- Are your motor symptoms well controlled? Poorly controlled motor symptoms such as tremor or stiffness can affect a person's self-perception with low self-esteem and also result in performance anxiety. Also, the bed partner might lose sexual interest.
- Are your mood symptoms well controlled? Depression and anxiety are common conditions in PD. They are known to be associated with a decrease in sexual function, notably a loss of libido. Discuss the pros and cons of treating those symptoms of your sexual function as some of the mainstay treatments can worsen sexual performance.
- Discuss medication options. Testosterone deficiency becomes more prevalent with age (and is common in PD), and a study has shown that replacing testosterone can improve some of the symptoms in people with PD. Also, women dealing with a decrease in sexual desire can use an FDA approved medication called Flibanserin. This medication has not been explicitly tested in people with PD. One large study (TEST-PD) did not find testosterone replacement useful for PD motor symptoms but sometimes it can help sexual symptoms.
- Consider a sex therapist. You might notice an improvement in your sexual life and satisfaction after consultation with a sex therapist. These are mental health counselors or psychologists who have received extra training to help people with sexual or intimacy problems. One of the Parkinson’s Foundation Centers of Excellence in Tel Aviv Israel has pioneered the use of a sex therapist on a multidisciplinary team.
Dr. Wissam Deeb is the co-author of the recent book, Living with Parkinson’s (Robert Rose, 2020).


To read more books and articles by Michael S. Okun MD check Twitter @MichaelOkun and these websites with blogs and information on his books and http://parkinsonsecrets.com/ #Livingwith Parkinson’s #EndingPD #Parkinsonsecrets #LessonBedside and https://www.tourettetreatment.com/
He also serves as the Medical Director for the Parkinson’s Foundation.
To see more on Dr. Indu Subramanian she does live interviews of experts in Parkinson’s for the PMD Alliance.
References:
Margolesky J, Betté S, Singer C. Management of Urologic and Sexual Dysfunction in Parkinson Disease. Clin Geriatr Med. 2020 Feb;36(1):69-80. doi: 10.1016/j.cger.2019.09.011. Epub 2019 Sep 10. PMID: 31733703.
Picillo M, Palladino R, Erro R, Colosimo C, Marconi R, Antonini A, Barone P; PRIAMO study group. The PRIAMO study: active sexual life is associated with better motor and non-motor outcomes in men with early Parkinson's disease. Eur J Neurol. 2019 Oct;26(10):1327-1333. doi: 10.1111/ene.13983. Epub 2019 Jul 2. PMID: 31267621.
Bronner G, Cohen OS, Yahalom G, Kozlova E, Orlev Y, Molshatzki N, Strauss H, Hassin-Baer S. Correlates of quality of sexual life in male and female patients with Parkinson disease and their partners. Parkinsonism Relat Disord. 2014 Oct;20(10):1085-8. doi: 10.1016/j.parkreldis.2014.07.003. Epub 2014 Jul 12. PMID: 25131540.
Ginsberg TB. Aging and sexuality. Med Clin North Am. 2006 Sep;90(5):1025-36. doi: 10.1016/j.mcna.2006.06.003. PMID: 16962855.
Yu M, Roane DM, Miner CR, Fleming M, Rogers JD. Dimensions of sexual dysfunction in Parkinson disease. Am J Geriatr Psychiatry. 2004 Mar-Apr;12(2):221-6. PMID: 15010351.