

Why you should take care of your bones if you have Parkinson's disease?

Are you thinking about your bone health in Parkinson’s? You should be! Picture by Jonny Acheson.
By Michael S. Okun
Parkinson’s disease is commonly accompanied by soft or brittle bones. Parkinson’s disease affects more men than women and people tend to forget about monitoring bone health in men with this neurodegenerative condition. In this month’s blog we will dig deep into the osteoporosis challenge in Parkinson’s disease. I will recommend proactive strategies you can use to strengthen your bones.
What is the most common bone abnormality in Parkinson’s and why do we care?
Following a bone scan many persons with Parkinson’s will be shown to have a reduction in their bone mass density. We care about the bone mass density because a low bone mass density is an important factor in how often a bone is broken. The mobility and balance challenges of Parkinson’s disease increase the risk of broken bones (fractures). You should therefore be ‘proactive’ about strengthening the bones if you have Parkinson’s.
What is the difference between osteoporosis and osteopenia?

Knowing about your bone health in Parkinson’s is critical and there are tests like a DEXA scan that can help you to be proactive and prevent soft bones. Nice example picture is located here: https://medizzy.com/feed/25384260
The terms are defined by the severity of bone loss and also by the risk of future bone fractures. Osteopenia is when the bone mineral density is lower than when compared to a normal person. Osteoporosis is when there is a significantly reduced bone mineral density along with weakened bone structure. A diagnosis of osteoporosis carries an increased risk of broken bones also referred to as fractures.
What are the risks to your bone health if you have Parkinson’s disease?

What do we know about bone health and Parkinson’s?
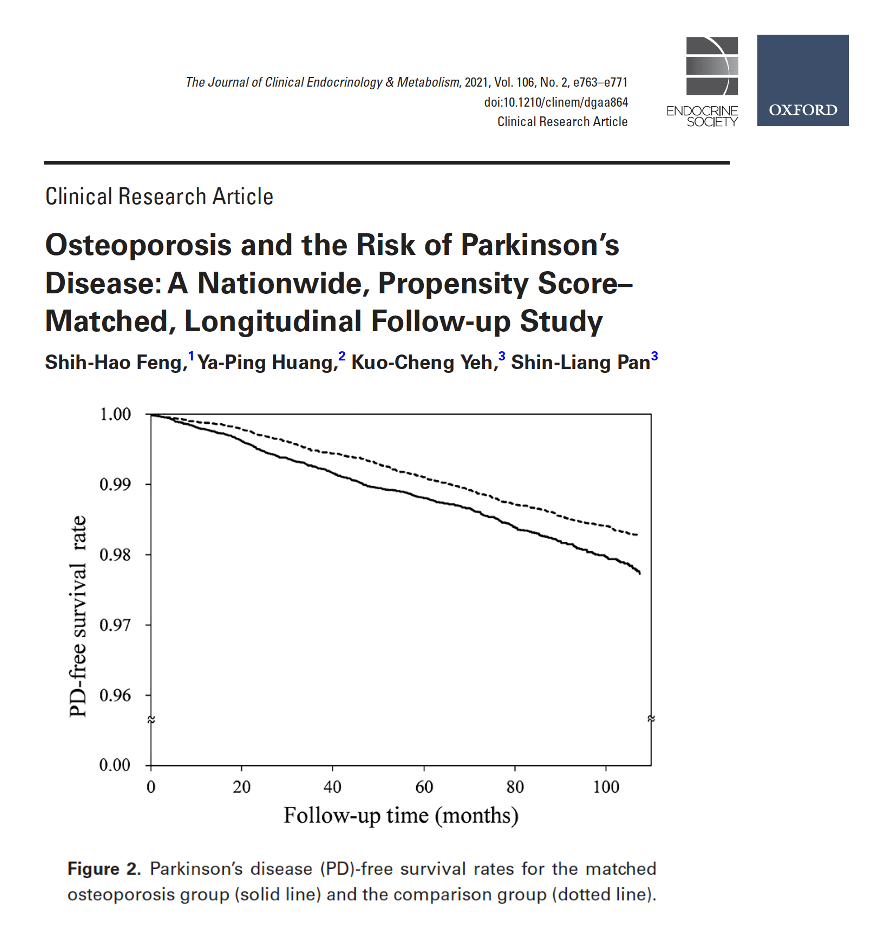
Torsney, Lees and colleagues explored the risks of bone health in Parkinson’s disease in their 2014 article. The authors reviewed 23 relevant studies and their results were published in the Journal of Neurology Neurosurgery and Psychiatry. The bottom line was that if you have Parkinson’s disease, the risk was much higher for osteoporosis (OR 2.61; 95% CI 1.69 to 4.03) and it was estimated to be DOUBLE when compared to a normal age matched population. The risk was present for both men and women with Parkinson’s disease, but was greater for women. Further, Parkinson’s had an increased risk for fractures (OR 2.28; 95% CI 1.83 to 2.83). Another study by Feng and colleagues in a Taiwanese cohort (2020) showed that those diagnosed with osteoporosis had a slightly elevated risk of later being diagnosed with Parkinson’s disease. They also showed a potential increase in mortality in those with Parkinson’s and osteoporosis.
What is the relationship between osteoporosis and Parkinson’s disease?
Should your fracture risk be assessed with a screening tool?
Yes. There are many simple screening tools which can be administered to determine your fracture risk. One commonly used international tool is called the FRAX. Unfortunately, the FRAX and other available tools do not specifically address Parkinson’s disease and Parkinson’s related falling.
What is a DEXA scan and why do I need one if I have Parkinson’s?

This is a nice example of a DEXA scan available on the UC Davis website.
A DEXA scan is called dual-energy X-ray absorptiometry. The test measures a your bone mineral density. Your doctor or health care professional will share the results with you in something called a T-score. A normal T-score is -1.0 or greater. If you have a diagnosis of osteopenia, the T-score will be between -1.0 and -2.5. Finally, if you have osteoporosis, the T-score will be -2.5 or lower.
Is a DEXA bone scan safe?
You should know that a DEXA scan is considered a safe and non-invasive procedure. It uses very low levels of X-ray radiation. The radiation levels are lower than in a common chest X-ray or a computed tomography (CT) scan. Experts have estimated that the dose of radiation from a DEXA scan is comparable to the radiation you receive during the course of a typical day. The scan takes about 20 minutes, and there are no injections, incisions or contrast agents. Pregnant women are advised to avoid DEXA scans (if possible).
What are the symptoms of osteopenia?
Frequently, this condition is asymptomatic and you would not know you have ‘soft bones’ without performing a test such as a DEXA scan.
What are the symptoms of osteoporosis?
Like osteopenia, osteoporosis can be invisible. If your healthcare team finds fractures in the hip, spine, or wrist, these may be important clues. Some folks with osteoporosis may lose height or take on a stooped posture. Since Parkinson’s can also be associated with loss of height and a stooped posture, screening with bone density scans is considered especially important.
What are the possible risk factors for bone loss?

The spinal vertebrae are filled with trabecular bone and the interconnections of the bone are important to maintain strength and prevent fractures.
Nice picture and description here: https://www.open.edu/openlearncreate/mod/oucontent/view.php?id=132819&printable=1
The risk factors for osteoporosis include aging, menopause, nutritional deficiencies and not walking enough (referred to by doctors as being sedentary. Smoking, drinking alcohol and taking corticosteroids can all put you at risk for soft bones. Osteopenia and osteoporosis have been shown to be associated with chronic illnesses such as Parkinson’s disease.

Cortical bone is made up of smooth layers of tissue as shown by this nice image found: https://www.open.edu/openlearncreate/mod/oucontent/view.php?id=132819&printable=1
Is your muscle health important to prevention of osteoporosis and osteopenia?

Lower lean appendicular mass has been associated with osteoporosis.
We think the answer is yes. Lima and colleagues, in a recent study, revealed an association between lower lean appendicular mass and osteoporosis. Most experts agree that paying attention to exercise, muscle mass and muscle quality will all be an important to your bone health in the setting of Parkinson’s disease. The authors of this study teach us that “muscles and bones share common anabolic pathways, and muscle-derived factors, such as irisin, (and these may) directly influence bone metabolism.”
How do you apply clinical practice guidelines for treatment of bone loss to Parkinson’s disease?

What happens to your bone as you age. Nice summary which shows men versus women: https://www.open.edu/openlearncreate/mod/oucontent/view.php?id=132819&printable=1
Mícheal Ó Breasail and colleagues recently performed a systematic review of the treatment of osteoporosis and osteopenia in Parkinson’s disease. The authors identified 6 relevant papers that contained recommendations for bone health in Parkinson’s disease and they addressed clinical practice guidelines, consensus statements, and treatment algorithms. Bone health was recognized as important by all 6 teams writing on this topic. The authors found it surprising that “recommendations for fracture-risk screening were inconsistent.” Only one paper addressed the “acceptability and tolerance of anti-osteoporosis medications” when administered in the setting of Parkinson’s disease. This paper did incorporate “national osteoporosis guidelines into a Parkinson’s disease specific treatment algorithm.”
Do brain degeneration and dopamine drugs contribute to bone loss in Parkinson’s disease?

Are experiments on mice telling us something about the effects of dopamine medications on bone health.
We think so. The degenerative process in Parkinson’s includes brain regions critical to brain related pathways that are important to bone health. Much of what we know today on this topic has been learned from animal experiments. In animals experiments, Handa and colleagues in a 2019 paper in the journal Scientific Reports, showed that bone metabolism can be mediated by the dopaminergic system and that hormones and administration of dopamine drugs play a role. Important work remains to be done to clarify the degenerative processes leading to bone loss and the effects of dopaminergic medications.
What are my treatment options if I have osteopenia or osteoporosis with my Parkinson’s?

Lifestyle change is the first place to start when addressing bone health in Parkinson’s. Nice article and picture at: https://www.verywellhealth.com/how-to-treat-osteoporosis-5206668
The best place to start for addressing osteopenia is to change lifestyle. Improving calcium and vitamin D intake are imperative, and adding weight-bearing and strength-training exercises can also be a critical component to avoid futher bone loss. If you smoke or drink it is time to consider quitting..
If you are diagnosed with osteoporosis, in addition to the above considerations, your health care professional should discuss the risks and benefits of bone strengthening medications including bisphosphonates, denosumab, and possibly hormone-related therapies.
What is known about the association between bone loss and Parkinson’s?
The degenerative brain process in Parkinson’s disease affects important circuitry for bone health. Many published studies have revealed a higher prevalence of osteoporosis and osteopenia in persons with Parkinson’s. The immobility and reduction in overall physical activity in the setting of Parkinson’s disease, place both men and women at risk. Additionally, vitamin D deficiency is common in Parkinson’s disease. Addressing vitamin D deficiency with sunlight is a double edged sword, as there is an increased risk of melanoma if you have Parkinson’s disease. Studies have revealed an altered metabolism of calcium which can reduce bone thickness. The Parkinson’s medications such as dopamine agonists have been thought to also reduce bone density. as dopamine has been shown to be important to remodeling of bone. Finally, a reduction in estrogen or testosterone levels also contributes to bone loss.
Researchers have been interested in whether inflammation can impact bone health in the setting of Parkinson’s. Experts have opined that it is possible that inflammation stimulates osteoclast activity (cells that break down bone) and inflammation reduces osteoblast activity (cells that make new bone).
What drugs have been associated with a potential risk of bone fractures?

Here is a nice table of some of the drugs listed in the publication US Pharmacist known to be associated with hip fractures. Another not listed are the drugs for gastroesophageal reflux. Here is a link to the article: https://www.uspharmacist.com/article/gastric-acid-suppressants-and-association-with-fractures-in-women
Drugs that have been associated with falls and fractures include antidepressants, dopaminergic drugs, drugs that block dopamine (neuroleptics), and benzodiazepines, along with other anti-anxiety agents. It is important that if you have Parkinson’s, you should appreciate that the association of these drugs does not automatically translate to the drugs ‘causing bone fractures.’
What are the drugs that can be used to address bone health in Parkinson’s and what are the challenges in using them?

Here is a list of some of the medication treatments for osteoporosis provided in this nice article at: https://www.uspharmacist.com/article/overview-of-the-management-of-osteoporosis-in-women
The swallowing challenges, along with slowed gut motility, and possible malabsorption should all be considered when choosing a drug to treat bone health in Parkinson’s disease.
There bone health drugs are called bisphosphonates and these can be taken each day in a pill or liquid formulation. These drugs include alendronate, ibandronate, and risedronate. Bisphosphonates stop the bone from being reabsorbed by the body. These drugs can prove challenging for people with Parkinson’s disease, as they must be taken early in the morning and only on an ‘empty stomach.’ Most prescribing healthcare practitioners recommend they not be taken with other medications, and this requirement can be challenging for those with Parkinson’s disease. Further, the requirement for a full glass of water and remaining upright and fasting for half an hour after each dose can be difficult if you have Parkinson’s disease.
One alternative approach to administering a bisphosphonate in Parkinson’s is by IV (intravenous). Zoledronic acid is administered once a year for three years. This approach has been associated with ~75% reduction in spine fractures and a 40% reduction in other fractures. Though data has been lacking specifically for Parkinson’s disease, there is a large ongoing multi-center trial on this drug.
An alternative medication approach has been using the drug Denosumab. This drug works on the immune system, and is called a monoclonal antibody. This drug is administered under the skin every six months, and should be avoided if you have kidney disease. One worrisome side effect may emerge when the drug is stopped, and it may lead to an unexpected rebound worsening in fractures.

Michael Okun is an American author, neurologist and researcher in Parkinson’s disease. He is the author of several books including Parkinson’s Treatment: 10 Secrets to a Happier Life, Ending Parkinson’s and the Parkinson’s Plan. He is the author of this blog post.

Jonny Acheson is a doctor, a person with Parkinson’s and our website artist.
Selected references:
Figueroa CA, Rosen CJ. Parkinson's disease and osteoporosis: basic and clinical implications. Expert Rev Endocrinol Metab. 2020 May;15(3):185-193. doi: 10.1080/17446651.2020.1756772. Epub 2020 Apr 26. PMID: 32336178; PMCID: PMC7250483.
van den Bos F, Speelman AD, Samson M, Munneke M, Bloem BR, Verhaar HJ. Parkinson's disease and osteoporosis. Age Ageing. 2013 Mar;42(2):156-62. doi: 10.1093/ageing/afs161. Epub 2012 Nov 6. PMID: 23132148.
Feng SH, Huang YP, Yeh KC, Pan SL. Osteoporosis and the Risk of Parkinson's Disease: A Nationwide, Propensity Score-Matched, Longitudinal Follow-up Study. J Clin Endocrinol Metab. 2021 Jan 23;106(2):e763-e771. doi: 10.1210/clinem/dgaa864. PMID: 33236101.
Kim TL, Byun SJ, Seong MY, Oh BM, Park SJ, Seo HG. Fracture risk and impact of osteoporosis in patients with Parkinson's disease: a nationwide database study. J Bone Miner Metab. 2022 Jul;40(4):602-612. doi: 10.1007/s00774-022-01322-w. Epub 2022 Mar 26. PMID: 35347431.
Tan YJ, Lim SY, Yong VW, Choo XY, Ng YD, Sugumaran K, Md Shah MN, Raja Aman RRA, Paramasivam SS, Mohd Ramli N, Grossmann M, Tan AH. Osteoporosis in Parkinson's Disease: Relevance of Distal Radius Dual-Energy X-Ray Absorptiometry (DXA) and Sarcopenia. J Clin Densitom. 2021 Jul-Sep;24(3):351-361. doi: 10.1016/j.jocd.2020.07.001. Epub 2020 Jul 30. PMID: 32888777.
Lima DP, Chagas-Neto FAD, Gomes de Luna JR, Martins YO, de Almeida SB, Feitosa CX, Gradvohl LB, Rosa ID, Lopes FKM, Aragão LFF, Viana-Júnior AB, Augusto KL, Roriz-Filho JS, d'Alva CB, Montenegro-Júnior RM, Braga-Neto P. Osteoporosis in Parkinson's disease and the role of lean body mass: a cross-sectional study in a Brazilian tertiary center. Front Endocrinol (Lausanne). 2024 Apr 22;15:1326212. doi: 10.3389/fendo.2024.1326212. PMID: 38711983; PMCID: PMC11070524.
Boelens Keun JT, Arnoldussen IA, Vriend C, van de Rest O. Dietary Approaches to Improve Efficacy and Control Side Effects of Levodopa Therapy in Parkinson's Disease: A Systematic Review. Adv Nutr. 2021 Dec 1;12(6):2265-2287. doi: 10.1093/advances/nmab060. PMID: 34113965; PMCID: PMC8634393.
Roy A, Naik D. Osteoporosis in Parkinson's Disease: In Search of the Best Prediction Tool. Ann Indian Acad Neurol. 2023 Jul-Aug;26(4):359-360. doi: 10.4103/aian.aian_400_23. Epub 2023 Sep 11. PMID: 37970315; PMCID: PMC10645269.
Invernizzi M, Carda S, Viscontini GS, Cisari C. Osteoporosis in Parkinson's disease. Parkinsonism Relat Disord. 2009 Jun;15(5):339-46. doi: 10.1016/j.parkreldis.2009.02.009. Epub 2009 Apr 5. PMID: 19346153.
Lee JY, Lim NG, Chung CK, Lee JY, Kim HJ, Park SB. Parkinson's Disease as Risk Factor in Osteoporosis and Osteoporotic Vertebral Fracture : Prevalence Study Using National Inpatient Sample Database in Korea. J Korean Neurosurg Soc. 2019 Jan;62(1):71-82. doi: 10.3340/jkns.2018.0012. Epub 2018 Dec 31. PMID: 30630295; PMCID: PMC6328797.
Xiong L, Pan JX, Guo HH, Mei L, Xiong WC. Parkinson's in the bone. Cell Biosci. 2021 Nov 5;11(1):190. doi: 10.1186/s13578-021-00702-5. PMID: 34740382; PMCID: PMC8569842.
Metta V, Sanchez TC, Padmakumar C. Osteoporosis: A Hidden Nonmotor Face of Parkinson's Disease. Int Rev Neurobiol. 2017;134:877-890. doi: 10.1016/bs.irn.2017.05.034. Epub 2017 Jul 10. PMID: 28805587.
Zhao Y, Shen L, Ji HF. Osteoporosis risk and bone mineral density levels in patients with Parkinson's disease: a meta-analysis. Bone. 2013 Jan;52(1):498-505. doi: 10.1016/j.bone.2012.09.013. Epub 2012 Sep 19. PMID: 23000281.
Zhang F, Lu J, Zhang Y, Liu J. Significance of non-motor symptoms and development of a screening tool for osteoporosis in Parkinson's disease. Clin Neurol Neurosurg. 2024 Apr;239:108181. doi: 10.1016/j.clineuro.2024.108181. Epub 2024 Mar 2. PMID: 38492436.
Park KY, Jung JH, Hwang HS, Park HK, Han K, Nam GE. Bone Mineral Density and the Risk of Parkinson's Disease in Postmenopausal Women. Mov Disord. 2023 Sep;38(9):1606-1614. doi: 10.1002/mds.29579. Epub 2023 Aug 21. PMID: 37602978.
Torsney KM, Noyce AJ, Doherty KM, Bestwick JP, Dobson R, Lees AJ. Bone health in Parkinson's disease: a systematic review and meta-analysis. J Neurol Neurosurg Psychiatry. 2014 Oct;85(10):1159-66. doi: 10.1136/jnnp-2013-307307. Epub 2014 Mar 11. PMID: 24620034; PMCID: PMC4173751.
Sato Y, Iwamoto J, Honda Y. Amelioration of osteoporosis and hypovitaminosis D by sunlight exposure in Parkinson's disease. Parkinsonism Relat Disord. 2011 Jan;17(1):22-6. doi: 10.1016/j.parkreldis.2010.10.008. Epub 2010 Nov 2. Retraction in: Parkinsonism Relat Disord. 2016 Jul;28:171. doi: 10.1016/j.parkreldis.2016.05.027. PMID: 21050796.
Henderson EJ, Lyell V, Bhimjiyani A, Amin J, Kobylecki C, Gregson CL. Management of fracture risk in Parkinson's: A revised algorithm and focused review of treatments. Parkinsonism Relat Disord. 2019 Jul;64:181-187. doi: 10.1016/j.parkreldis.2019.03.021. Epub 2019 Apr 8. PMID: 30992234.
Handa K, Kiyohara S, Yamakawa T, Ishikawa K, Hosonuma M, Sakai N, Karakawa A, Chatani M, Tsuji M, Inagaki K, Kiuchi Y, Takami M, Negishi-Koga T. Bone loss caused by dopaminergic degeneration and levodopa treatment in Parkinson's disease model mice. Sci Rep. 2019 Sep 24;9(1):13768. doi: 10.1038/s41598-019-50336-4. PMID: 31551490; PMCID: PMC6760231.
Feng SH, Huang YP, Yeh KC, Pan SL. Osteoporosis and the Risk of Parkinson's Disease: A Nationwide, Propensity Score-Matched, Longitudinal Follow-up Study. J Clin Endocrinol Metab. 2021 Jan 23;106(2):e763-e771. doi: 10.1210/clinem/dgaa864. PMID: 33236101.